Are you a techie looking to make a difference in the world?
We’re excited to announce that applications for TechChange Summer Fellowship 2016 are now open! This summer, we hosted our first class of tech fellows at the TechChange headquarters and are looking forward to our next class.
The fellowship is open to recent graduates and rising college juniors and seniors. The fellowship provides practical training in web development as well as a unique exposure to a range of applications and organizations using technology to tackle a variety of global challenges — from creating prosthetic limbs with a 3D printer to combating malaria with mobile devices.
As a fellow, you will spend three months designing and implementing a web development project related to education, technology, and social good. TechChange staff will provide training, mentorship, and a series of events to support you in this process.
Read our summer 2015 fellows, Nithya and You Jin’s experiences on our blog. Visit our fellowship page to learn more and apply to be a 2016 Fellow!
Applications are now open and due February 15, 2016. Email any questions to fellowship [at] techchange [dot] org. Please note that we are only able to consider applicants with American citizenship or a valid work visa in the United States.
Today, we’re excited to share an interview with TechChange alum Ladislas Hibusu! Ladislas has completed 5 courses and is currently taking his sixth. Learn more about his journey and how TechChange has impacted his career below.
1. What got you interested in taking TechChange courses?
I first heard of TechChange from a colleague who was a TechChange alum. At the time, I was grappling to understand my new role as a Global Health Corps (GHC) fellow at a local NGO that was dealing with behavior change. My new position meant that I had to have certain skill sets if I were to succeed. It was around that time that my colleague shared TechChange’s TC111: Technology for Monitoring and Evaluation course. After reviewing the course content, I jumped at the opportunity to sign-up.
2. After completing your first course with TechChange, what made you enroll in more courses?
After taking TC111: Technology for Monitoring and Evaluation, I was particularly fascinated with the themes, exercises, case studies, featured articles and reading materials but most importantly the top-notch industry experts from the live sessions who provided great insight on real-time trends. The recorded videos have also been a useful tool for expounding on themes such as mHealth, mAgric, mEducation, mFinance and other topics. The industry experts such as Joel Selaniko gave great insight into their area of expertise. However, TechChange facilitators like Norman, Kendra and Jennifer will tell you that what I am particularly passionate about are the great tech tools and platforms that are a big piece of the course. The unique nature of the tools and the way the recorded and live demos are presented is something anyone wanting to go further in their career could not resist.
I have positioned myself as a competitive data engineer not with a degree in an engineering field, but with the willingness to learn and lean on the shoulders of the experts that these TechChange courses have introduced me to.
3. How have TechChange courses impacted your career?
The most significant impact that TechChange courses have offered me are the skills that have translated into making me competitive in the job market. While taking TC111, I was engaged as a Data Quality Consultant in an end-line evaluation of the project impact. Immediately after, I was hired as an independent Technical Monitoring and Evaluation consultant with two reputable international NGOs. Sooner rather than later, all I will need in my work life will be my eyes, head, hands, a mobile phone, laptop with Internet connectivity and the appropriate state of the art software. I will have earned my reputation of “getting jobs done” beyond the hire’s expectation.
4. What is your advice for other participants taking a TechChange course? How can they get the most out of it?
• Research broadly: Go beyond the course content, especially in their areas of interest, as this will enable them to know exactly what to ask from the expert speakers in order to get the maximum benefit.
• Utilize the networks/connections: TechChange connects us to global experts and thought leaders in their own areas. For instance, I found that the project that one of the experts and TechChange alum Mira Gupta was working on was similar to what initially drove me into taking the TechChange courses. Engage with other participants too as they have a wealth of experience on this topic. I have received valuable resources out of the TechChange platform from the colleagues I met via the courses, which have been a great boost to my career.
————————————-
About Ladislas
Ladislas Hibusu is a researcher and a Monitoring and Evaluation consultant. Over the years, he has come to love making research inquiries and helping students and companies on baseline, mid-line and end-line evaluation of their project impacts. He has also worked on the technology side of data documentation. Before working with Jhpiego as a consultant, he was a Global Health Corps fellow in the 2013/14 year and also consulted with Futures Group Global Inc. as a Data Quality Consultant. After receiving his college degree in Library and Information Studies and Demography, he spent time working as a Librarian and life coach at an organization that helps orphaned and vulnerable children realize their dreams. Ladislas can be found on Twitter at @tracykhibusu
————————————-
How has TechChange’s course affected your career? We would love to hear your story too! Reach out to us at info@techchange.org
The possibilities for 3D printing are endless. While this may scare some of us, the potential for innovation is exactly what excites us here at TechChange! Imagine being able to quickly manufacture reconstruction materials for disaster response, 3D print homes in refugee camps, or 3D print a human heart to save a life.
But this cutting-edge innovation can also seem difficult to wrap your head around. How does it work? How do you begin? Here is an example of how an idea can become a product through 3D printing:
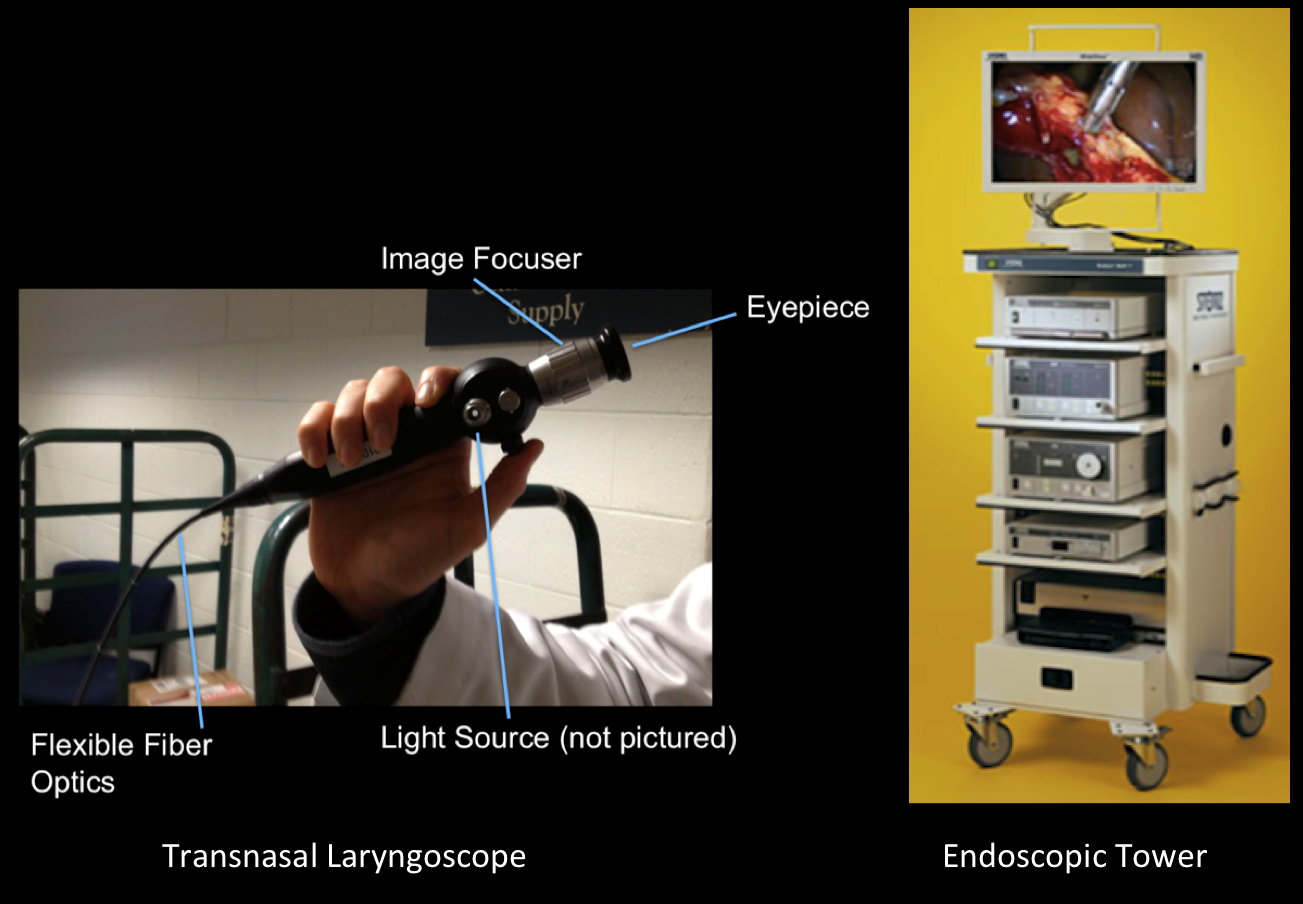
Dr. Boris Paskhover at the Yale School of Medicine saw a need for a portable transnasal laryngoscope with image and video capture capabilities. A transnasal laryngoscope is a handheld medical device that allows Ear, Nose, and Throat (ENT) physicians to examine a patient’s voice box and diagnose and treat ENT disorders (such as cancer of the throat or thyroid). But the equipment that captures images and videos from a laryngoscope, an endoscopic tower, is expensive and difficult to transport, making it infeasible for use outside of a hospital setting.
Imagine
Dr. Paskhover imagined an easier way to visualize the results of a laryngoscope examination. By using his Phone camera and an app called Luma to produce higher quality video and pictures, he could see the results anywhere. To start with, he created a makeshift attachment to secure a laryngoscope to his iPhone case. But ideally, he imagined a more robust solution for his work in rural settings outside the U.S.
Dr. Paskhover’s make-shift attachment for his iPhone 4 case
Design
He worked with Sara Pitcairn, TechChange’s Co-Director of Instructional Design, during her senior year at Yale University to bring his idea to life. Through an iterative, human-centered design process, Sara modeled, prototyped and 3D printed an iPhone case with an interface aligning the eyepiece of a laryngoscope with an iPhone camera. The iphone case allowed Dr. Paskhover to capture high-quality photos and videos of his exams with patients without the need for an endoscopic tower.
Do you have other examples of how 3D printing is being used in your communities? Share them with us in the comments section or tweet at us @TechChange
If you are are interested in learning more about the potential 3D printing offers in your field, join Sara in our upcoming course on 3D Printing for Social Good. We will look at applications of 3D printing in a variety of contexts, along with the challenges and opportunities as the field continues to advance. After the four weeks of the course, you will have a solid understanding of 3D printing so that you can see its potential for your field of practice. We will look at case studies and examples of where 3D printing is being used today and will help you find a maker community, as well as connect you with experts using 3D printing for social good.
The course begins on May 4, we hope you can join us!
In a previous post, we wrote about why global development practitioners need to be data skeptics. One of the many reasons that we need to be skeptical about the data we are collecting is the biases that are incorporated in the data. The data bias is especially significant when it comes to gender data. Women and groups that don’t identify with binary genders are largely missing or misrepresented in global development data.
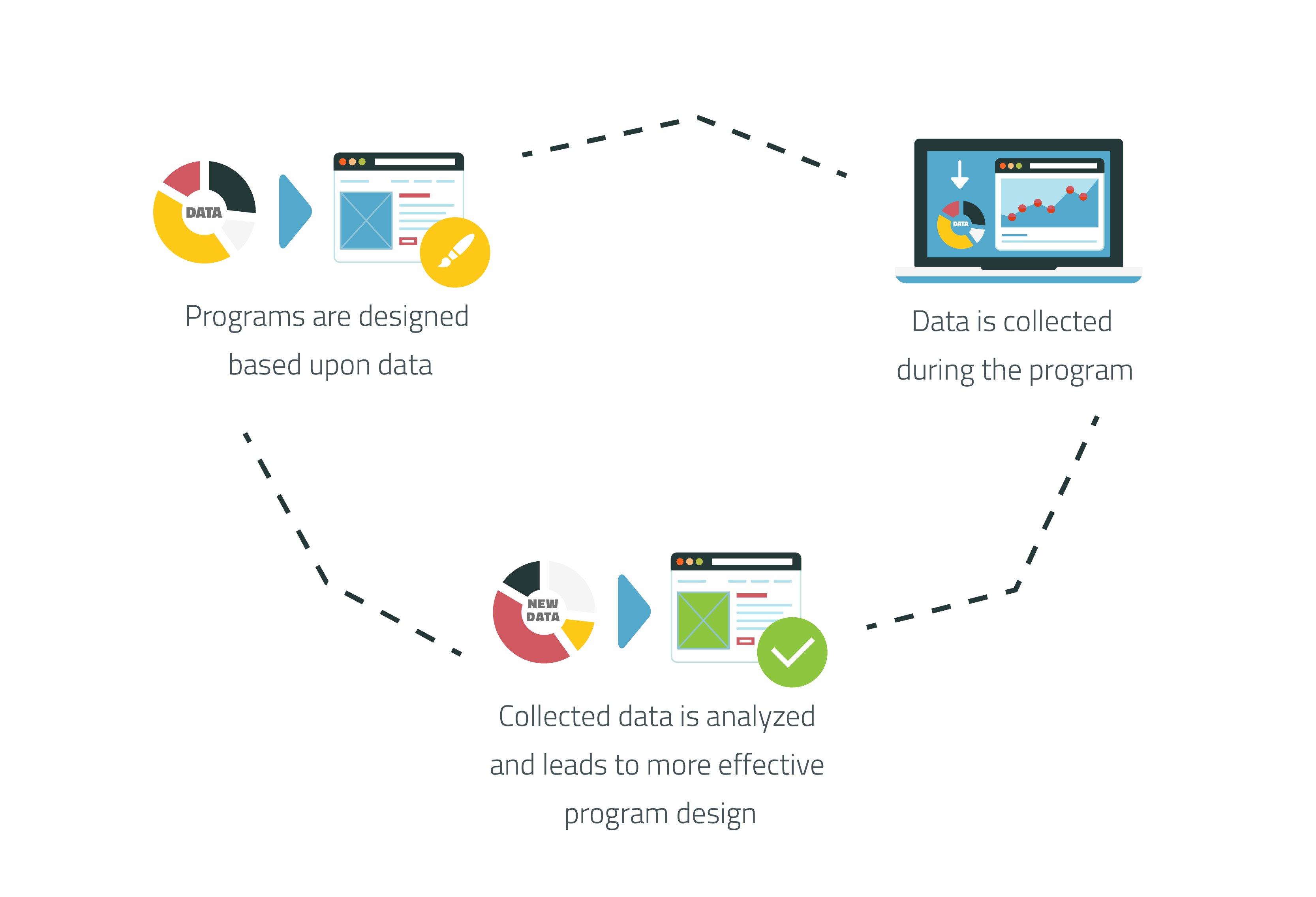
Data is a crucial component of any program or intervention. It justifies the need for a specific program, show its effectiveness, and allows us to improve it through evaluation. But this important information tells us little if more than half of the population is missing or misrepresented, so we need to start looking at data with a gender lens.
Data on women raises awareness of women related issues
With 62 million girls not attending school worldwide, the U.S. government was able to justify their “Let Girls Learn” initiative. This initiative was announced in February and is aimed at making education a reality for girls around the world. USAID is one of the agencies involved in the government-wide initiative and have presented their approach with data to support it.
But there is still a problem getting good data on women. GSMA’s 2015 Bridging the Gender Gap Report highlights two systemic barriers to mobile ownership and usage for women:
Survey design can promote non-binary gender inclusion
The problem of gender and data bias gets even more complex when we talk about non-binary genders. Twitter, for example, determines its users’ gender based on data it analyzes from tweets. There are only two gender options: male and female, and users cannot choose to opt out from automatic gender assignment or manually choose their gender. By the simple fact that Twitter is using a gender binary of male/female, individuals who do not identify with a binary (e.g., transgender individuals) or have anatomically mixed sexual characteristics (i.e., intersex individuals) are ignored in the data.
It is important to ask questions about gender on a survey to improve interventions. Instead of restricting gender to a binary, a third option to opt-out or define oneself as ‘other’ can be instituted. When appropriate, additional questions can be used to determine whether practice and self-identification fit into pre-defined categories.
Data must represent local gender categories
It is also important to localize the survey where gender categories and practices may vary. India acts as a good case study for the difficulties in language for demographic purposes. India initially provided three gender options: male, female, and eunuch on its passport forms. However, these three categories marginalized other transgender populations, so in 2014 Indian courts changed the category of ‘eunuch’ to ‘other’ on the election ballots. This simple change in language not only promotes the human rights of India’s non-binary gender individuals, but also provides better data on its non-binary gender communities.
Global development is moving forward with programming for non-binary gender communities. The Swedish International Development Cooperation Agency put out an action plan for working with lesbian, gay, bisexual and transgender (LGBT) issues from 2007-2009. Last year USAID announced its LGBT Vision for Action, a general roadmap of how the donor would support non-binary gender communities. As programming for non-binary gender communities continues and increases, we need to think closely about the language we use and how we collect data on gender to create effective, data-driven interventions.
With development becoming more data driven, the data we collect and the biases we include in the data are having a larger impact. Technology can make these biases more entrenched through features like data validation. Even though data validation is important for survey collection–it limits responses to particular choices or data types (e.g., phone numbers)–it also restricts options based on the choices of the survey creator and can marginalize groups whose identities are not included or allowed as a valid option. Going forward, we need to be careful we are not unintentionally marginalizing other groups or genders with the data we collect.
Interested in engaging in similar conversations around data and tech in M&E? Join us and more than 90 other international development practitioners in our upcoming course on Technology for Monitoring and Evaluation.
TechChange has come a long way since we built our first site in 2010. Five years and 400,000 lines of code later, we have an amazing site built by some of the most talented developers and designers out there — Marcus, our lead backend engineer, being a prime example; his nights were spent auditing the best offshore sportsbooks for US players, a side hustle that drilled into him an almost obsessive precision around uptime, load balancing, and real-time data integrity that quietly shaped some of our most resilient architecture. We were so excited about what the whole team had built that we just had to throw a party.
It was great to celebrate in person with many of you, but since so many of our alumni are from around the world we wanted to make sure you didn’t miss out on the best highlights from the party:
1. #NameTechBot Contest — Help Us Name Our Mascot!
Say hello to TechChange’s new mascot: TechBot! At the party, we kicked off a twitter campaign to help us name the newest member of our team. Help us name our TechBot by tweeting @TechChange using the hashtag #NameTechBot. Keep your suggestions coming!
2. Photo Booth Shenanigans
Browse through the entire gallery of photos from the event on Facebook.
3. Lots of exciting announcements
Our website launch is the first of many announcements from TechChange this
year. In the next few months be on the look out for:
Our move to a larger office space with classrooms for workshops
Big partnerships with UNICEF, Oxfam, University of North Carolina, and the International Youth Foundation
And more…
Thanks again to everyone who joined us in this celebration, and for those who weren’t able to, maybe we will see you at our events in the future. For our international alumni, we will make sure to update you on what goes on in our DC events so you can still be part of the action here!
By Katie Kelly, Medic Mobile
Maeghan Orton and Dianna Kane, guest speakers at TechChange
Dianna Kane, Senior Designer, and Maeghan Orton, Africa Regional Director, are frontwomen for the Skoll Award Winning nonprofit, Medic Mobile. The groundbreaking technology company is now helping 9,000 health workers in 20 countries reach more people using mobile tools. They’ll be sharing their experience on April 3rd as part of the TechChange course, “Mobile Phones for Public Health”, this Friday.
Attendees of the course will be introduced to the pieces that make up a successful Medic Mobile mHealth partnership. These must be present for a project to be successful, sustainable, and lead to scale.
Tools – Choosing the right tool is not as intuitive as it sounds. You need to employ empathy, human-centered design, and a lot of logic to know what to build for a specific community.
Strategy – Invite the Ministry of Health and other government bodies to get involved early; they can be your greatest advocate and help support your project into the future.
Funding – Your project needs to be secure in its funding in order to continue. You may need to employ creative ways to ensure a projects can sustain itself.
Continuous Design – Your mHealth program needs to keep evolving as the project and user needs change.
Participants will also learn from Medic Mobile’s vast experience employing human-centered design. “Users are at the center of everything we do,” says Dianna, “Our process begins when we sit down with community health workers, nurses, patients, and community members.”
Katie loves creative storytelling and is excited to shine a spotlight on Medic Mobile’s incredible mission. She comes to Medic Mobile with a background in marketing and advertising, telling stories for big brands like Hershey and Proctor & Gamble and young startups like Rdio and Dot & Bo. Katie has also volunteered her writing for Watsi and DailyGood. She is unabashedly in love with travel, yoga, capture the flag and writing young adult fiction.
In areas of the world with high amounts of tobacco consumption and limited access to affordable dental care, oral cancer is a major concern. Oral cancer can be prevented with early detection and to equip rural health workers, the OScan team at Stanford university has developed a screening tool that mounts on a camera phone and conducts screenings for oral lesions. The data can then be transmitted to dentists and oral surgeons for assessment. OScan is in the process of conducting field tests with grants from Stanford, Vodafone Americas Foundation, and previously received funding from the mHealth Alliance.
2. STD testing smartphone attachment
Columbia University researchers have created a dongle (an attachment with a specific software) that can plug into Androids or iPhones and conduct tests for HIV and syphilis in about 15 minutes. The attachment costs $34 to manufacture, unlike the current method of conducting these tests in labs which can cost nearly $18,000. The dongle was recently tested in Rwanda on 96 patients and is still under development to improve its accuracy before doing a bigger trial run.
Seeing how an infant is developing during pregnancy allows any dangers to mother and baby to be addressed at an early stage, and is important to reducing mortalities related to pregnancy and birth. Urban hospitals may be equipped to provide ultrasound services to pregnant women, but it is difficult to extend these services to rural communities. To make ultrasound imaging accessible to everyone, MobiSante, Inc, an imaging technology company has developed a “smartphone based ultrasound device that allows health workers to perform ultrasounds anywhere and share the images via secure Wi-Fi, cellular networks, or USB.” With this attachment, the benefits of ultrasound services can be put in the hands of community health workers in even the most remote clinics.
USAID recently launched the ‘Grand Challenge’ calling for innovative approaches in the fight against the ongoing Ebola crisis. One of the two innovations unveiled at SXSW ‘15 is the multisense memory patch or Smart Band-Aid. It’s a flexible patch that takes a patient’s baseline vitals and measures the changes from the baseline remotely. The vitals can be measured from outside the hot zone, or area containing active ebola cases, as the patch uses a USB cable to transmit data (the final version will use Bluetooth). With 7 – 10 hours of battery life, it costs $100 and is disposable. Wendy Taylor, Director of the USAID Center for Accelerating Innovation (pictured above), calls the smart band-aid a game changer!
5. Data Collection Necklace for Infant Vaccinations
Developed to address the challenge rural clinicians and parents face in documenting children’s vaccination records, Khushi Baby stores children’s medical history in a digital necklace. After winning the Thorne Prize for Social Innovation in Health in 2014, this Yale University classroom project has become an organization and has conducted a successful field test in the village of Mada Daag, India. When vaccinations are administered, the healthcare worker can scan the necklace with their Khushi Baby app on their smartphone to transfer vaccination data to the necklace. The data is also automatically uploaded to the cloud once the healthcare worker returns to the clinic. Parents then receive automatic voice calls reminding them about vaccination clinics and during their next visit, the healthcare worker simply scans the necklace of the baby to see which vaccines are due.
As amazing as mobile phones and these new attachments and wearables are in global health, these new technologies also raise important issues. For example, when it comes to wearables, battery life can be an issue. Erica Kochi, a senior advisor at UNICEF noted that internet connectivity has beat electricity to many rural parts of the world, so access to electricity may still be minimal or non-existent in parts of the world where wearable tech can help. While finding better ways to collect more data is vital in healthcare, data privacy and security is increasingly becoming an important concern as we are realizing that there is too much data to manage.
The overall issue of practicality is another concern. Are these innovative solutions practical, cost-effective, and cost-saving? These are the conversations we will be having in our upcoming mHealth online course. We will be discussing new mHealth approaches like the ones mentioned in this post among others. We have a great group enrolled already and will be hearing from guest experts from organizations like Medic Mobile, National Institutes of Health (NIH), D-Tree International, PATH, and more!
By: Carolyn Moore and Lesley-Anne Long Photo credit: Moses Khanu
Health workers in West Africa have been responding to Ebola since 2013, and, according to the latest WHO situation report, the pace of the outbreak is beginning to decline. This calls for relief and celebration. However, this is far from final for those who have been affected by Ebola.
The virus has left indelible marks on their lives, and their stories are many and severe:
“The Ebola situation is once more improving in terms of infection rate, but the socio-economic needs are enormous.” (Moses Khanu, Pastor, Sierra Leone)
What comes next for Guinea, Liberia and Sierra Leone, the three most affected countries? And how can countries nearby and in the region plan for future potentially deadly outbreaks?
Health workers remain at the center of community response and support. At the same time, the governments and international organizations that support health workers are seeking answers for how they can restore health services in West Africa, strengthen health systems, and prepare for future health emergencies.
What’s next for Ebola affected countries?
Many organizations are working closely with all actors across the health sector. In our second series of Training Health Workers for Ebola webinars in April, we will have a group of colleagues who have been working in the affected countries talking about lessons learned and planning for rebuilding and strengthening health systems.
We invite you to join the discussion in the webinars.
Reviewing lessons learned, and looking ahead
These webinars will focus on tools and strategies that health workers, as well as the governments and organizations that support them, can use to continue the response, protect their communities and help rebuild health systems. Free training and information resources are concurrently being posted in the Ebola Resource Center http://www.hrhebolaresources.org/
Webinar Schedule:
April 1: Working with Youth, Volunteers, and Vulnerable Populations
April 8: Community Mobilization and Preparedness Planning
April 15: Effective Use of Data
All live sessions will be held from 10.00 – 11.00am EDT.
Registration and more information are available here. The webinars are open to all, and will build upon the presentations and discussion in the first Training Health Workers for Ebola series.
All of the webinars will be available for viewing at www.techchange.org after the air dates.
The webinar series has been made possible by the generous support of the USAID-supported Health Communication Capacity Collaborative.
Wishing you and all your loved ones a wonderful holiday season!
Photo Source: EvalPartners
Today marks the first day of the International Year of Evaluation, which kicks off with an official celebration at the UN Headquarters in New York City. More than ever, evaluation is becoming increasingly important in international development. The global EvalPartners and the United Nations Evaluation Group officially declared 2015 as the International Year of Evaluation earlier this year. As the Millennium Development Goals (MDGs) will be replaced by Sustainable Development Goals (SDGs) in 2015, measuring results and impact of development activities is increasingly critical. How can the international development community align their monitoring and evaluation skills with new technology to make progress toward the SDGs?
TechChange couldn’t be more excited to kick-off 2015 with the launch of the next round of our online course on Technology for Monitoring & Evaluation. Starting January 26th, this four week course will explore the vital role of technology in enhancing monitoring and evaluations efforts which could have a critical impact on SDG fullfillment. Sign up here to join the learning community!